The SCS system stimulates the dorsal column of the spinal cord by tiny electrical impulses from small electrical wires placed on the spinal cord. This pain modality offers an option to patients with chronic back pain, and can be particularly helpful in patients with chronic leg pain that is unresponsive to other medical treatment.
Spinal cord stimulation consists of one or two lead wires with a number of electrodes and a pulse generator or battery. The lead wire carries the electrical stimulation from the pulse generator or battery to the posterior column of the spinal cord.
The mechanism of spinal cord stimulation is still unknown. Some believe that stimulation of the dorsal columns closes the ‘gates’ to pain transmission, while others believe that pain relief from SCS results from direct inhibition of pain pathways in the spinothalamic tracts rather than being due to selective large
fiber stimulation. The other possible mechanism of SCS might involve producing supraspinal pain inhibition, activation of central inhibitory mechanisms influencing sympathetic efferent neurons, and activation of neurotransmitters or neuromodulators.
There are two different types of SCS system, one that is totally implantable and another with an internal SCS lead and an external RF transmitter. An external RF system might be best for the patient who requires a higher voltage or a multilead therapy for pain relief. The power source can be externally worn on a patient’s belt to transmit RF energy to the pulse generator that is implanted subcutaneously. The internal battery needs to be surgically replaced every 2–5 years, depending on usage. The SCS leads can be placed into the epidural space either percutaneously or with a small laminotomy.
Indications
Patient selected for SCS should be free of drug dependence, be psychologically suitable and stable, and be a highly motivated individual. The specific types of conditions considered for SCS include radiculopathy, failed neck or back syndrome, epidural fibrosis or arachnoiditis (resulting in radiculopathy), postherpetic neuralgia, peripheral neuropathy, intercostals neuralgia, complex regional pain syndromes.
Technique:
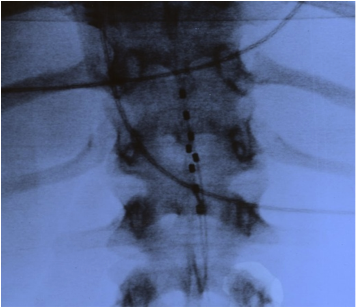
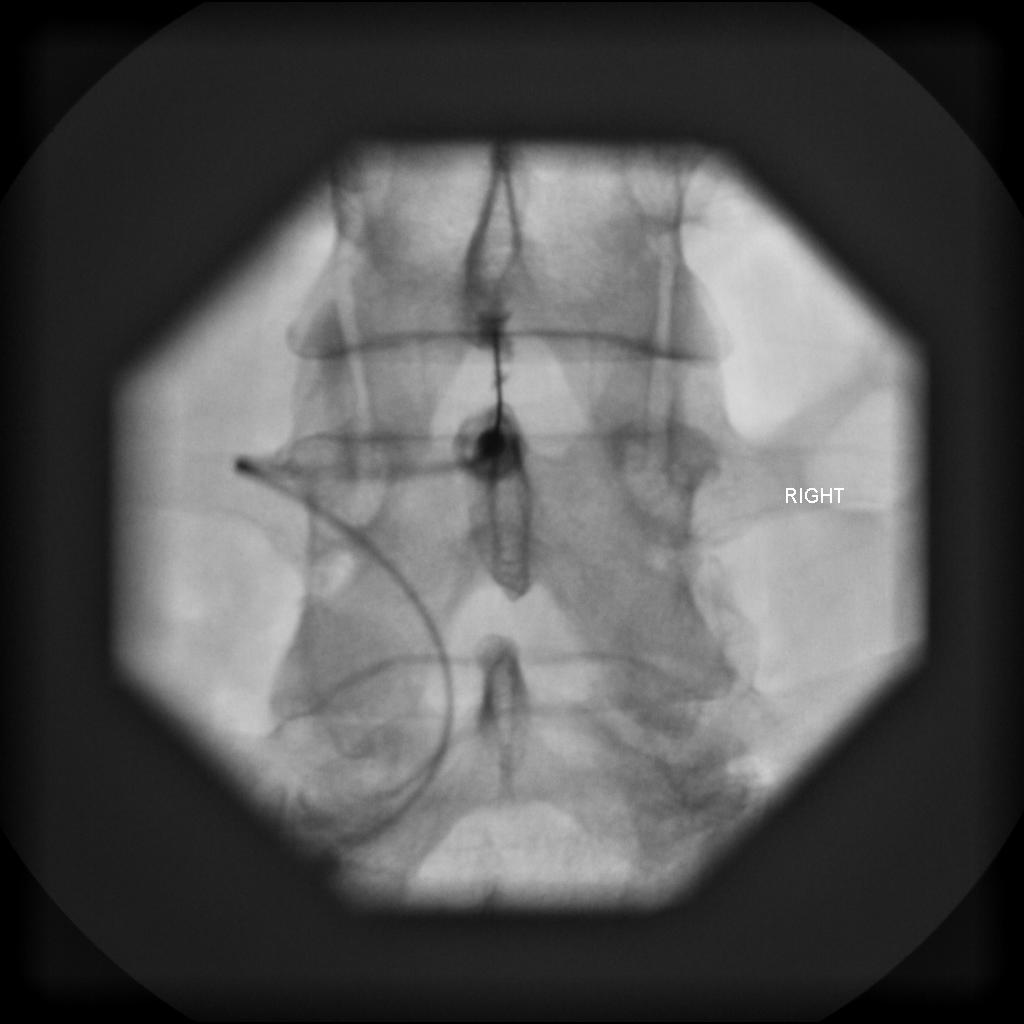
The patient is placed in a modified lateral decubitus position. A large-gauge epidural needle is advanced under AP fluoroscopy into the T12–L1 interlaminar space using a loss of resistance technique. The needle enters at an angle of approximately 30° from horizontal. The syringe is removed after entering the epidural, and an SCS lead is passed through the needle into the epidural space. The lead is advanced under fluoroscopic guidance, steering it by alternately rotating the needle or lead as well as advancing or retracting the lead, being careful not to shear off the lead into the epidural space.
The SCS lead tip should be placed at the top of T9 (for lumbar coverage) or the top of C3 (for cervical coverage). The lead should be placed either in the midline for a bilateral stimulation pattern or to the symptomatic side for a unilateral stimulation pattern. The patient is then sent home for a trial stimulation for no less than 2 days and typically for 5–7 days.
If the trial was satisfactory, then the patient is scheduled for a permanent SCS.
The permanent placement procedure is very similar to that used for temporary placement. Once the lead is in place, it is permanently attached to the supraspinous ligament or fascia. The battery or RF receiver is then implanted into the fatty layer of the lower abdomen, or one of the buttocks, through a small incision.