Vertebroplasty is a minimally invasive procedure for the treatment of pain and instability caused by a vertebral body compression fracture. The term vertebroplasty refers to percutaneous structural reinforcement of the compressed vertebral body using polymethylmethacrylate acrylic cement.
The cement hardens on delivery into the vertebral body, providing support and stabilization of the vertebral fracture, or compression by eliminating micromovement of the fracture fragments. Nevertheless, the main goal of vertebroplasty is pain relief from the compression fracture by either stabilizing the fracture or destroying pain fibers from its exothermic reaction.
Kyphoplasty was developed to restore vertebral height and spinal alignment that is not possible with vertebroplasty. Kyphoplasty involves placing a catheter with a balloon tip through a large gauge size needle into the vertebral body. The balloon is then inflated, which partially restores vertebral height and
creates a cavity for cement injection. The balloon is deflated and removed, after which the cement is injected into the vertebral body. In addition to restoring vertebral height and spinal alignment, kyphoplasty allows for the injection of cement under low pressure, potentially reducing the risk for cement extrusion.
Inclusion criteria:
• Patients with osteoporotic compression fractures, from 2 weeks old up to 1 year.
• Spinal compression fracture secondary to metastatic tumor
• Benign spinal tumors such as hemangiomas
Exclusion criteria:
• Infection such as discitis, osteomyelitis, or sepsis.
• Compromise of the spinal canal by retropulsed bone fragments
or tumor
• Fracture older than 2 years, greater than 75% collapse of the vertebral body, disruption of the posterior vertebral body wall, and fractures above T5
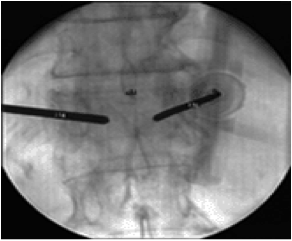
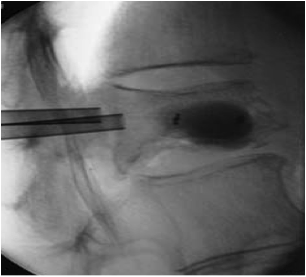
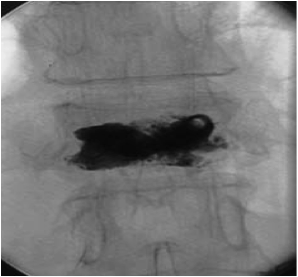
Technique:
The patient is placed in the prone position, and the C arm is rotated to maximize the oval appearance of the pedicle. The C arm is then tilted to obtain a sharp view of the vertebral end plates. A large-gauge needle is inserted at the center of the pedicle under fluoroscopy, and then advanced through the pedicle. The needle is kept parallel to the pedicle, and a lateral fluoroscopic view is obtained while the needle is advanced into the anterior third of the vertebral body using a twisting motion or gentle tapping of the needle with a sterile hammer. The needle stylet is removed, and 2-3 mL of the contrast dye is injected into the vertebral body, followed by injection of 3–5 mL of the cement. The injection is stopped when the cement spreads into the posterior third of the vertebral body. The stylet is placed back into the needle and the needle is removed from the vertebra. Vertebroplasty can be performed using either a single or a bilateral pedicular method depending on the degree of vertebral filling with the cement.