Facet syndrome is characterised by Stiffness and pain in the back, with pain in buttocks and thighs developing by prolonged sitting and standing for more than 6 months with no response to conservative treatment, and the primary source of pain was confirmed to be lumbar zygapophyseal joints.
Technique:
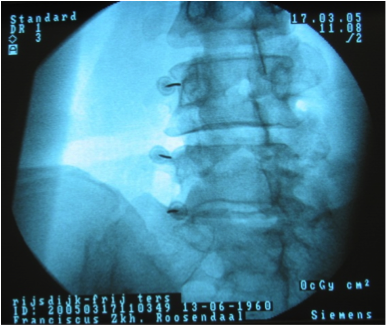
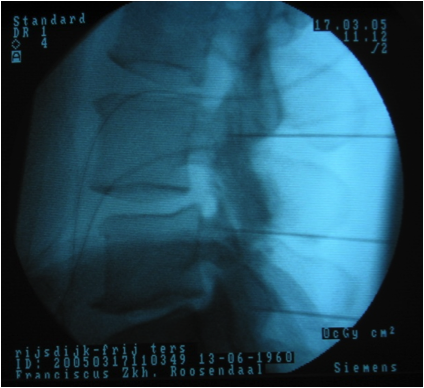
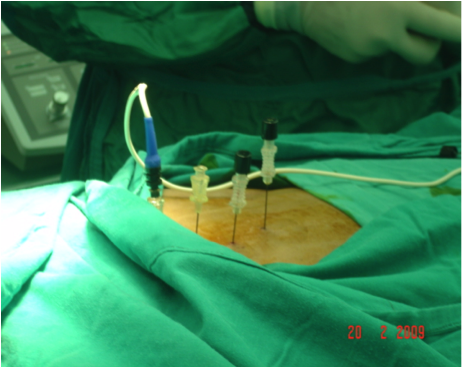
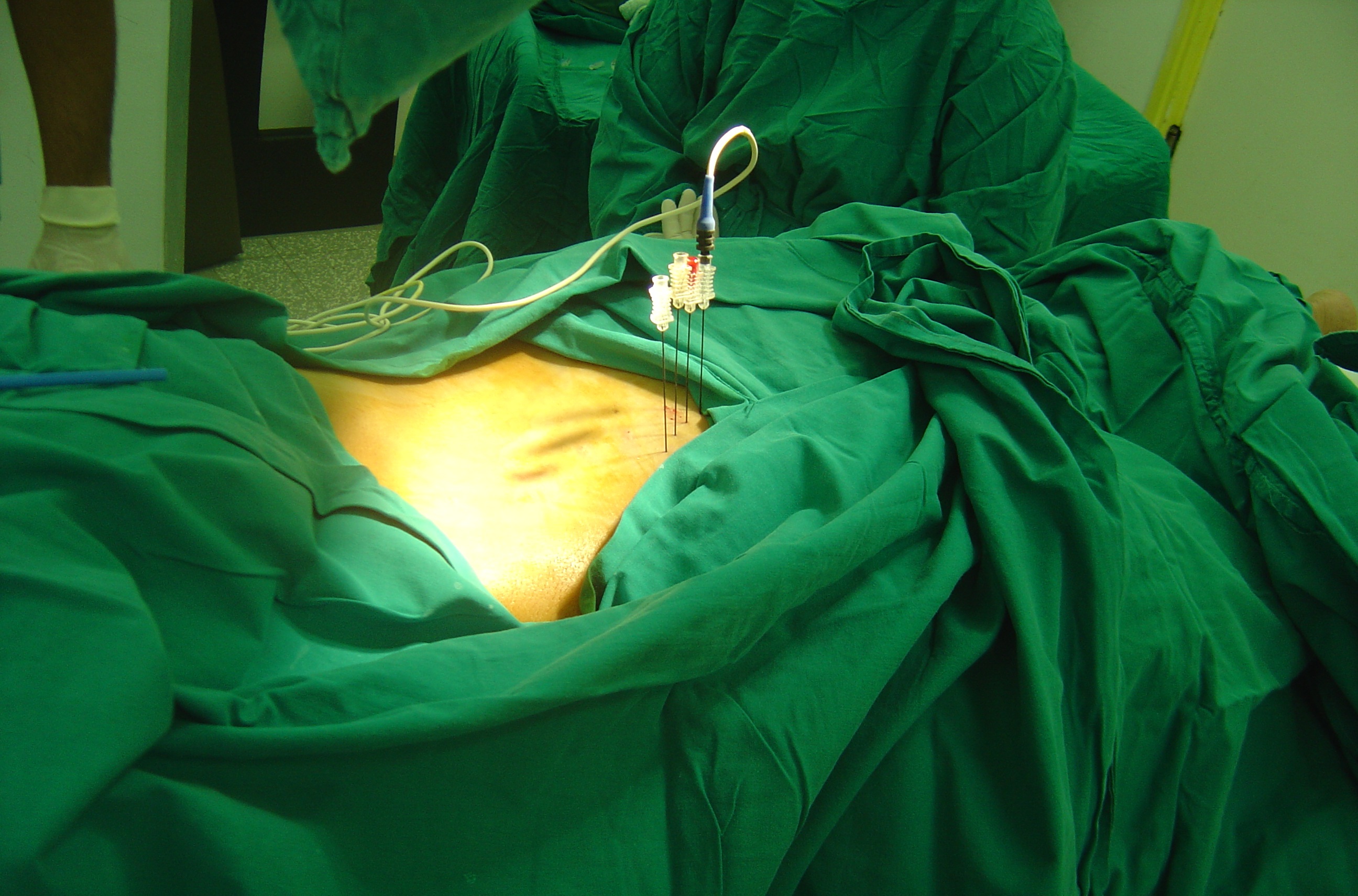
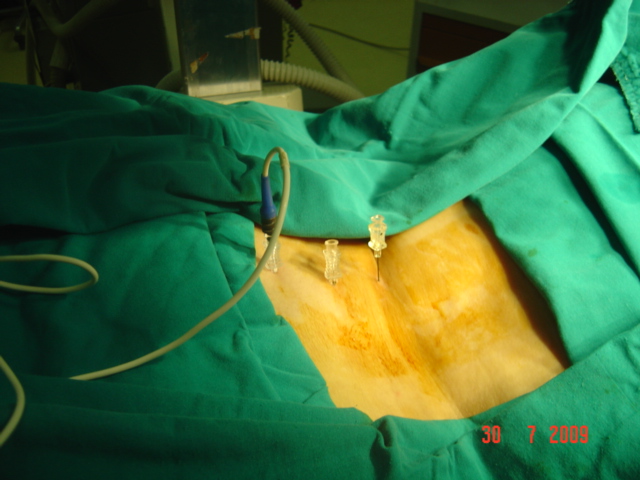
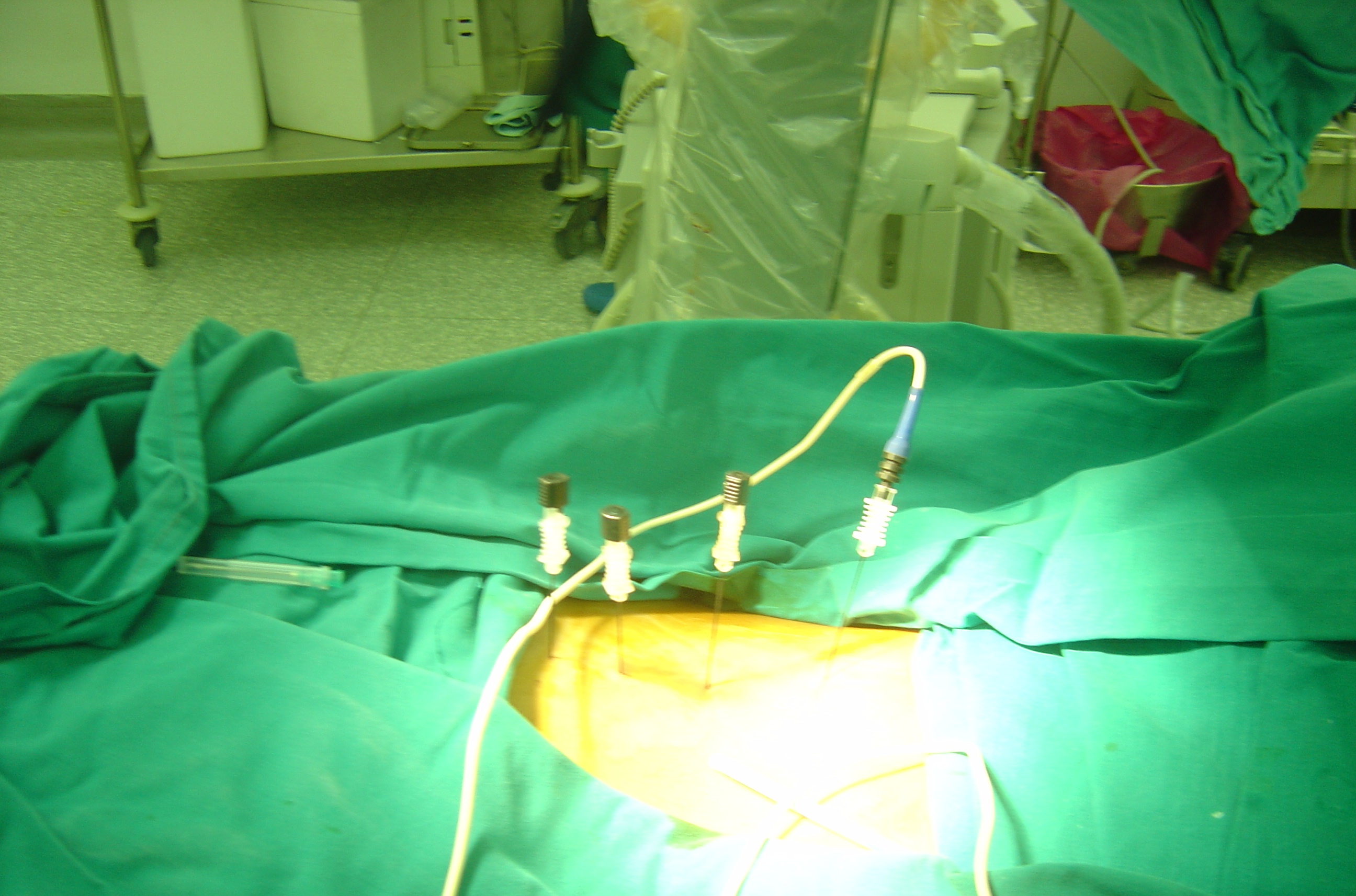
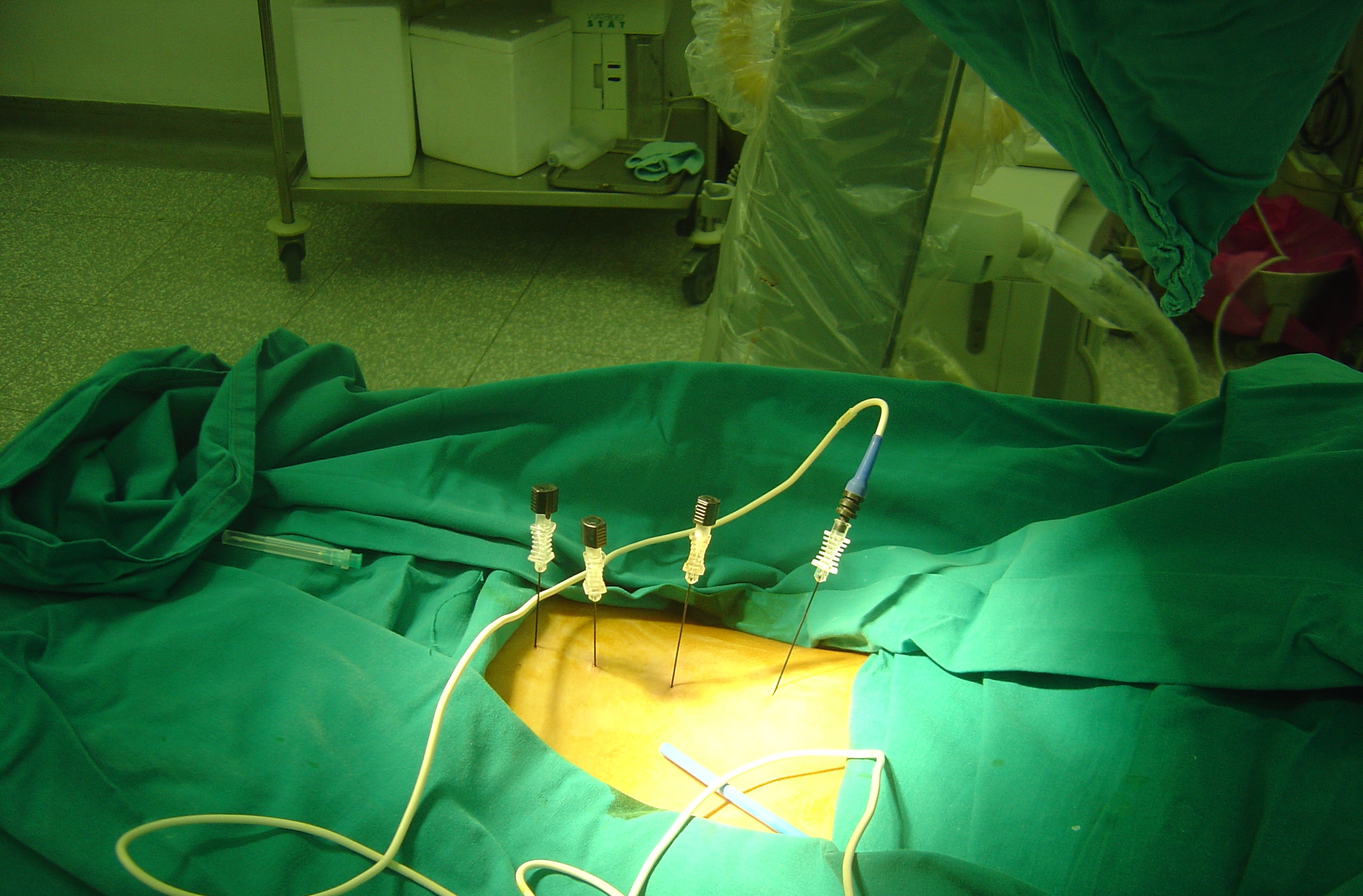
The Patient is placed in the prone position, with the fluoroscopic beam is directed at 30° in oblique direction, and the needle target and entry site should be at the “eye” of the “Scotty dog,” just a few milimeters caudally from the projection of the transverse process and superior articular process (SAP) junction.
Sensory and motor stimulation is performed as a safety precaution and to improve the success rate of the procedure.
The voltage at which the patient first perceives the stimulation in the appropriate dermatome is the sensory threshold. This threshold is usually around 0.4–0.7 V when the tip of the needle is next to the medial branch nerve using a frequency of 50 Hz. The frequency is changed to 2 Hz for motor stimulation, and the voltage intensity has to increase to at least twice the sensory threshold before motor activity in the myotomal distribution is typically seen.
Lesion is created at 80 degree for 60 seconds for each level.
The patient is complaining of pain and stiffness in the back, with pain radiating to the buttocks and thighs developing by prolonged sitting and standing for more than 6 months. The procedure is performed in an outpatient setting. The treatment is done with local anesthesia along with IV sedation when needed .The Patient is placed in the prone position, with the fluoroscopic beam is directed at 30° in oblique direction, and the needle target and entry site should be at the “eye” of the “Scotty dog,” . The Needle placement is confirmed with anterior–posterior (AP) imaging. Sensory and motor stimulation is performed as a safety precaution and to improve the success rate of the procedure. The medial branch nerve is anesthetized before Radiofrequency lesioning at 80–90°C for 30 s to 2 min per lesion. The needle was removed and puncture site was sterilized and covered.