Patients will present with a severe, unilateral, pulsatile, periorbital pain that typically lasts anywhere from 20 minutes to 3 hours. Patients may also experience tearing from the eye on the same side of the head as the pain as well as nasal discharge or stuffiness.
Cluster headache & Atypical facial pain:
Cluster headache is a disease that involves, as its most prominent feature, repeated attacks of excruciatingly severe pain that occur always on only one side of the head. (Unilaterally). Cluster Headache belongs to a group of primary headache conditions. There is currently no known cure for cluster headache.
Cluster headaches often occur periodically; spontaneous remissions may interrupt active periods of pain, though about 10-15% of chronic cluster headache sufferers never remit. The cause of the condition is not yet known. It affects approximately 0.1% of the population and men are more commonly affected than women.
Cluster headaches are recurring bouts of excruciating unilateral headache attacks of extreme intensity. The duration of typical cluster headache attack ranges from about 15 to 180 minutes. The onset of an attack is rapid and most often without the preliminary signs that are characteristic in migraine. Some sufferers report preliminary sensations of pain in the general area of attack, often referred to as “shadows”, that may warn them an attack is lurking or imminent, or may linger after an attack has passed, or between attacks. Though cluster headache is strictly unilateral, there are some documented cases of “side-shift” between cluster periods, or even rarer, simultaneously (within the same cluster period) bilateral headache.
Cluster headaches have been historically classified as vascular headaches. For decades, it has been proposed that intense pain was caused by dilation of blood vessels which was thought to create pressure on the trigeminal nerve. While this theory was thought to be the immediate cause of the pain, the etiology is not yet fully understood and cluster headache pathogenesis still remains the subject of ongoing research and debate.
There’s no cure for cluster headaches. The goal of treatment is to decrease the severity of pain, shorten the headache period and prevent the attacks.
Technique:
The sphenopalatine ganglion, which is located just behind the maxillary sinus, behind the cheek, can carry the pain information for multiple disorders, including atypical facial pain, post herpetic neuralgia, trigeminal neuralgia, migraine headaches, and cluster headaches.
All patients were provided informed consent before undergoing the procedure. The patient was placed in a supine position with the head extended by placing a soft rolled towel interscapular. The procedure was performed under intravenous sedation (Fentanyl and Propofol). Electrocardiogram and pulse oximetry and blood pressure readings were obtained for continuous hemodynamic monitoring and patients received a prophylactic antibiotic intravenous (third generation cephalosporin) 1 hour before the procedure.
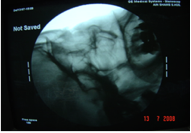
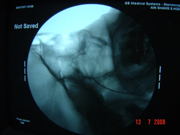
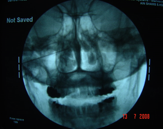
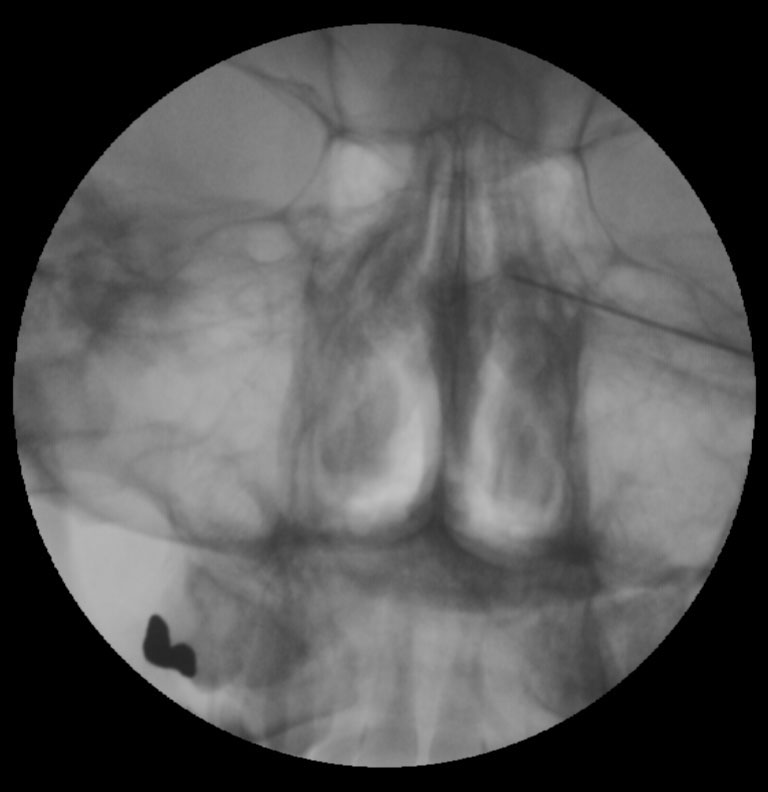
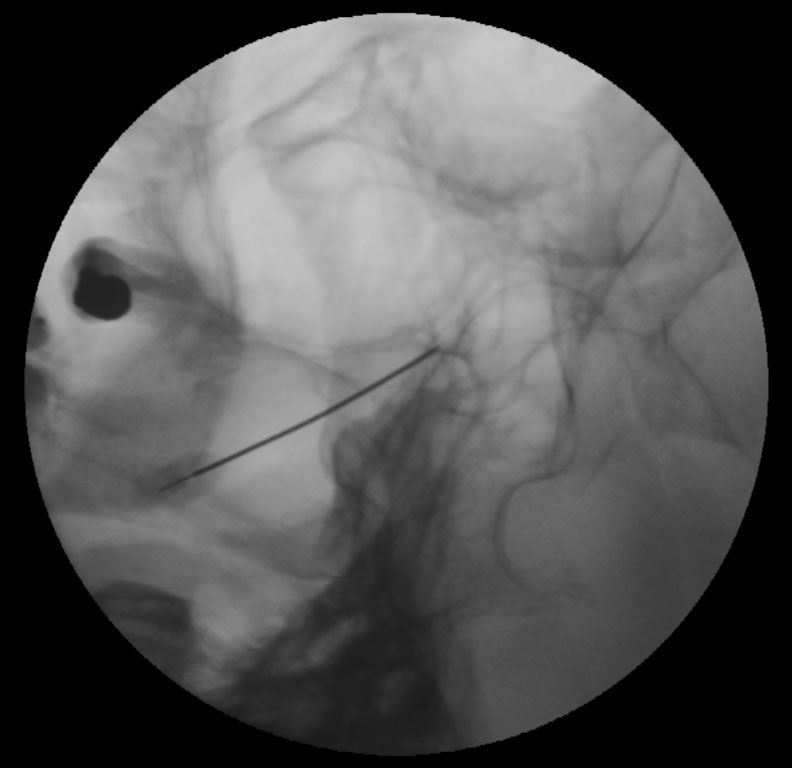
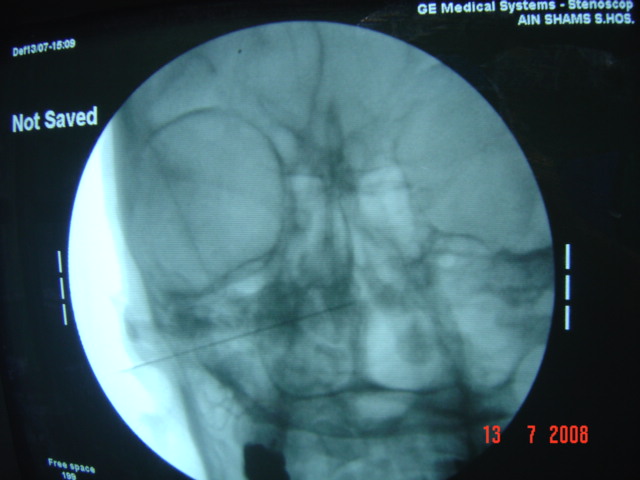
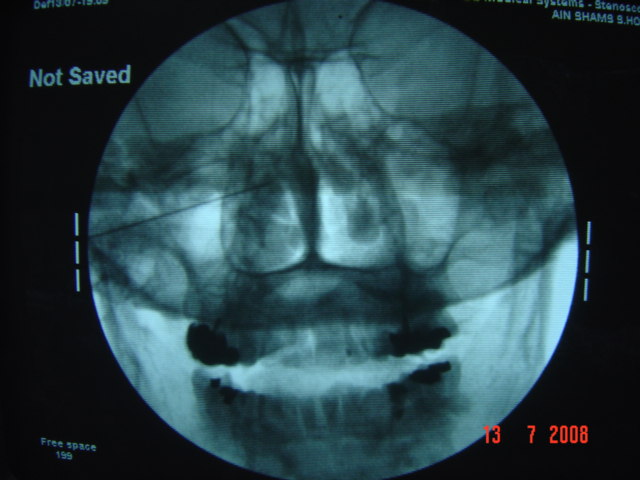
The procedure is performed under fluoroscopic guidance with the patient in the supine position and head extended. The needle is advanced slowly in the mandibular notch under x-ray guidance toward the pterygomaxillary fissure.
Once the needle entered the pterygomaxillary fissure, the C-arm was then rotated laterally to ascertain the depth of penetration inside the sphenopalatine ganglia. Sensory and motor stimulation is carried out at 50 Hz and 2 HZ respectively. Radiofrequency lesioning is then applied for 6 minutes at 45 V, with a pulse width of 10 ms and a pulse frequency of 4 Hz. The cut-off needle tip temperature was set at 42 ∞C.
The needle was then removed and the patients were discharged home within 4 to 6 hours after the procedure. The patients received oral antibiotic for 5 days. Patients were allowed to return to work on the second day following the procedure.