Hyperhidrosis, which is sweating in excess of that required for normal thermoregulation, is a condition that usually begins in either childhood or adolescence. Although any site on the body can be affected by hyperhidrosis, the sites most commonly affected are the palms, soles, and axillae. Hyperhidrosis may be idiopathic or secondary to other diseases, metabolic disorders, febrile illnesses, or medication use. Hyperhidrosis exists in 3 forms: emotionally induced hyperhidrosis (in which it affects the palms, soles, and axillae, localized hyperhidrosis, and generalized hyperhidrosis. Hyperhidrosis often causes great emotional distress and occupational disability for the patient, regardless of the form.
Indication for Sympathectomy.
Hyperhidrosis represents an idiopathic disorder of autonomic function that causes excessive perspiration. Its cause is unknown.
Complex Regional Pain Syndrome compasses a variety of painful conditions that follow tissue injury (trauma and infection), appears regionally, has a distal predominance of abnormal findings, exceeds in magnitude and duration the expected clinical course of the inciting event, often results in significant impairment of motor function, and shows variable progression over time
Limited cases of vasculitis caused by distal embolization or arteriosclerotic occlusive disease e.g. Raynaud’s disease.
Patients with severe unremitting pain, narcotics (Whether oral, parentral, or intraspinal) often inadequately relieve pain, and the progression of the malignant disease shorten the life expectancy of the patient
Because of the inaccessibility of the sympathetic chain, a great variety of surgical techniques have been described for sympathetic denervation. As none invasive approaches (Medical treatment), minimally invasive approaches (Endoscopic sympathectomy and Percutaneous Sympathicolysis), and invasive approaches (open surgical sympathectomy).
These minimally invasive techniques for sympathetic denervation appear to have a low morbidity and shorter hospital stay than for open surgical approaches. Patient demand and improved satisfaction with shorter hospital stays that reduce costs now make these minimally invasive techniques for sympathectomy an attractive alternative of choice to treat sympathetically mediated syndromes
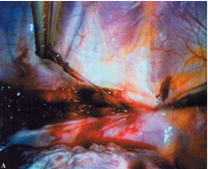
The patients were offered to choose between thoracoscopic sympathectomy and percutaneous radiofrequency ablation of the thoracic sympathetic chain. As regard thoracoscopic sympathectomy, it was done unilateral on the same session under general anesthesia. There were wound incisions and postoperative pain as compared between with percutaneous radiofrequency ablation of the thoracic sympathetic chain which was done under local anesthesia and sedation, no incisions, but the procedure was done only unilateral on the session.
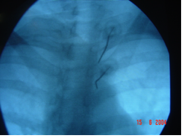
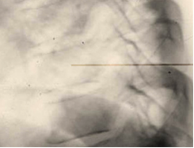
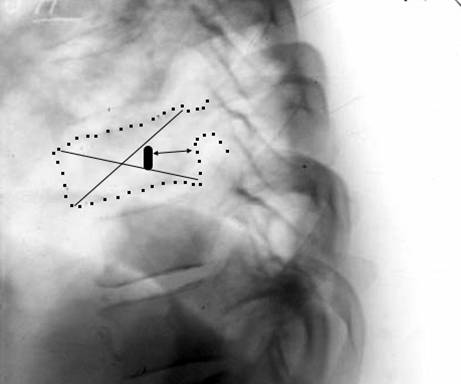
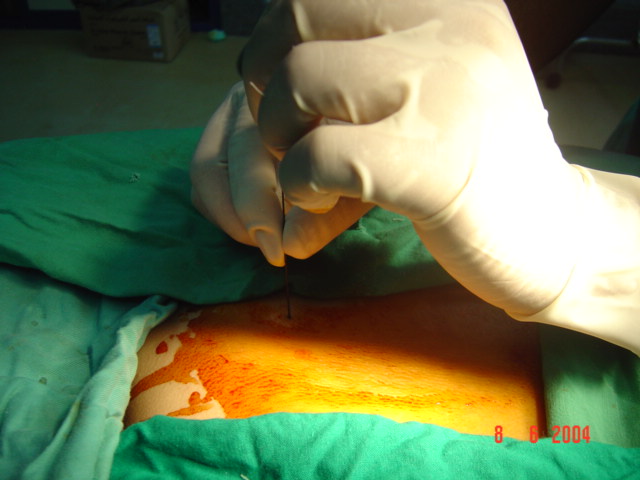
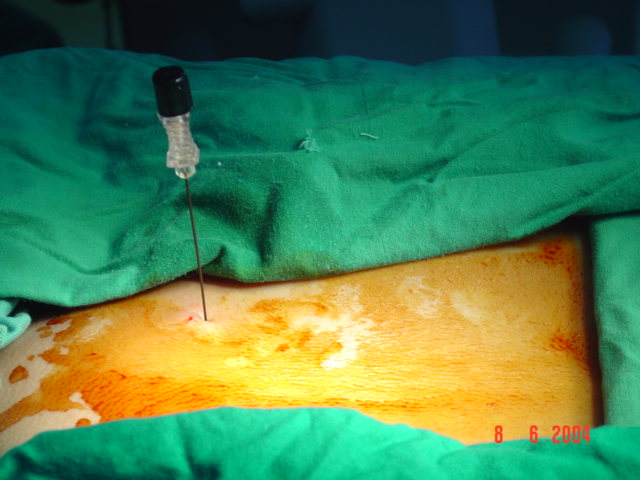
The patient is complaining of sweating in excess of that required for normal thermoregulation. Hyperhydrosis is a condition that usually begins in either childhood or adolescence. Although any site on the body can be affected by hyperhidrosis, the sites most commonly affected are the palms, soles, and axillae. The procedure is performed in an outpatient setting. The treatment is done with local anesthesia along with IV sedation when needed. The Patient is placed in the prone position, with the fluoroscopic beam is directed at craniocaudal direction, and the needle target and entry site should be at the middle of the second and third thoracic vertebral body . The Needle placement is confirmed with anterior–posterior (AP) and lateral imaging. Sensory and motor stimulation is performed as a safety precaution and to improve the success rate of the procedure. The sympathetic chain is anesthetized before Radiofrequency lesioning at 80–90°C for 2 min per lesion. The needle was removed and puncture site was sterilized and covered.